



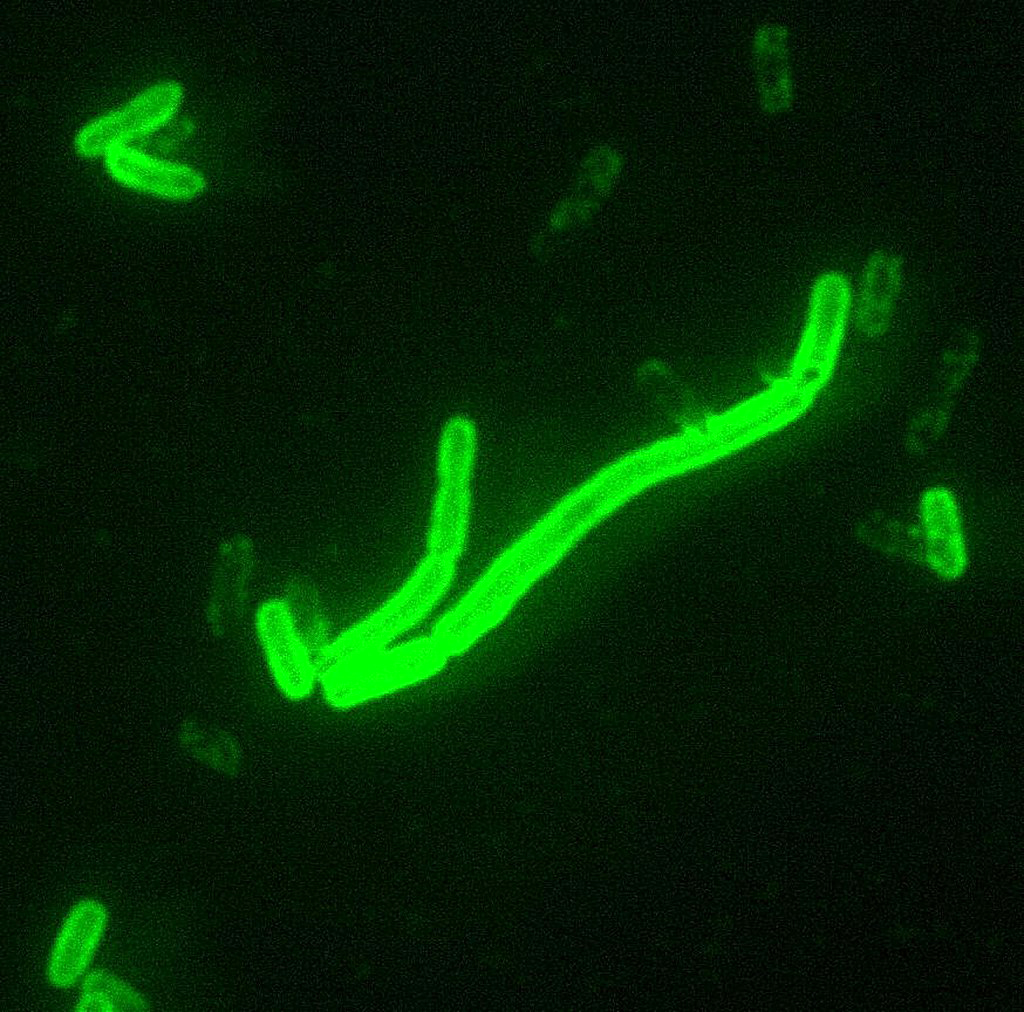




Plague is an infectious disease caused by the bacterium Yersinia pestis.
♦ Signs and symptoms
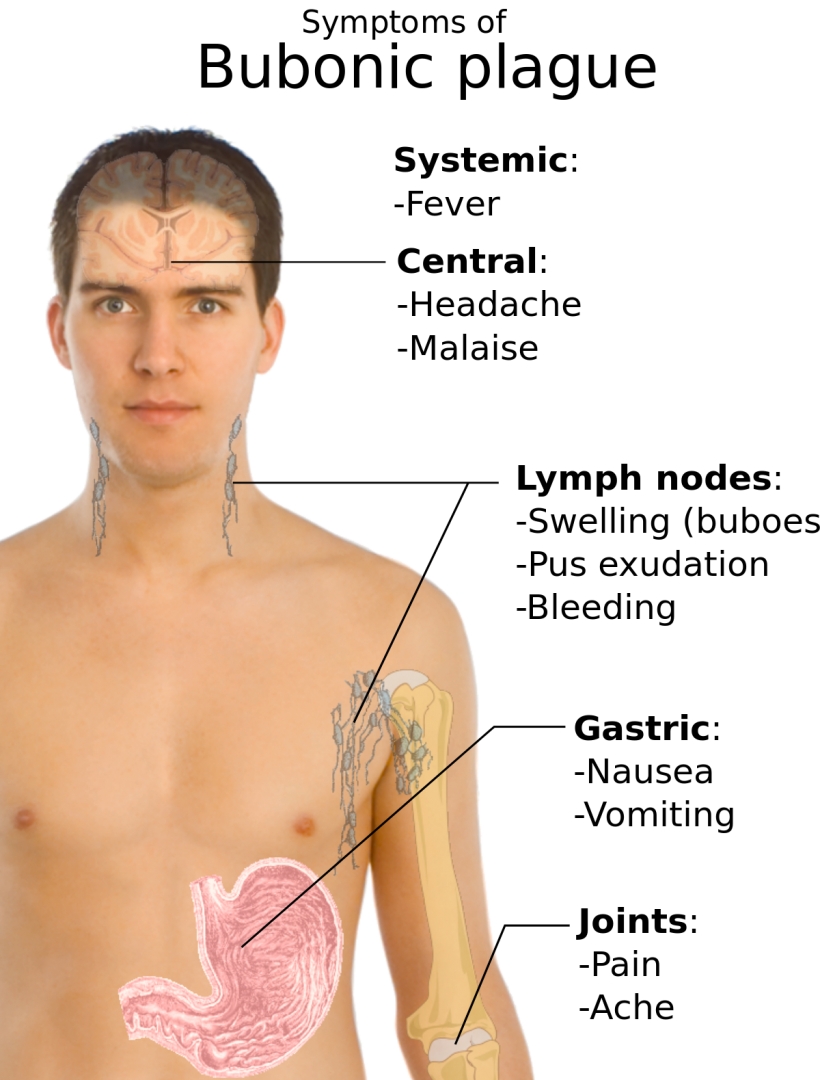
General symptoms of plague include fever, chills, headaches, and nausea.
Many people experience swelling in their lymph nodes if they have bubonic plague.
For those with pneumonic plague, symptoms may (or may not) include a cough, pain in the chest, and haemoptysis.
Other clinical manifestations include plague meningitis, plague pharyngitis, and ocular plague.
There are three forms of plague, each affecting a different part of the body and causing associated symptoms.
- Bubonic plague affects the lymph nodes, making them swell
- Septicemic plague infects the blood and can cause tissues to turn black and die.
- Pneumonic plague infects the lungs, causing shortness of breath, coughing and chest pain
- Bubonic plague
Swollen inguinal lymph glands on a person infected with the bubonic plague.
The swollen lymph glands are termed buboes from the Greek word for groin, swollen gland: bubo.
When a flea bites a human and contaminates the wound with regurgitated blood, the plague-causing bacteria are passed into the tissue.
Y. pestis can reproduce inside cells, so even if phagocytosed, they can still survive. Once in the body, the bacteria can enter the lymphatic system, which drains interstitial fluid.
Plague bacteria secrete several toxins, one of which is known to cause beta-adrenergic blockade.
Y. pestis spreads through the lymphatic vessels of the infected human until it reaches a lymph node, where it causes acute lymphadenitis.
The swollen lymph nodes form the characteristic buboes associated with the disease, and autopsies of these buboes have revealed them to be mostly hemorrhagic or necrotic.
If the lymph node is overwhelmed, the infection can pass into the bloodstream, causing secondary septicemic plague and if the lungs are seeded, it can cause secondary pneumonic plague.
- Septicemic plague
Lymphatics ultimately drain into the bloodstream, so the plague bacteria may enter the blood and travel to almost any part of the body.
In septicemic plague, bacterial endotoxins cause disseminated intravascular coagulation (DIC), causing tiny clots throughout the body and possibly ischemic necrosis (tissue death due to lack of circulation/perfusion to that tissue) from the clots. DIC results in depletion of the body's clotting resources so that it can no longer control bleeding.
Consequently, there is bleeding into the skin and other organs, which can cause red and/or black patchy rash and hemoptysis/hematemesis (coughing up/ vomiting of blood).
There are bumps on the skin that look somewhat like insect bites; these are usually red, and sometimes white in the centre.
Untreated, the septicemic plague is usually fatal.
Early treatment with antibiotics reduces the mortality rate to between 4 and 15 per cent.
- Pneumonic plague
The pneumonic form of plague arises from infection of the lungs.
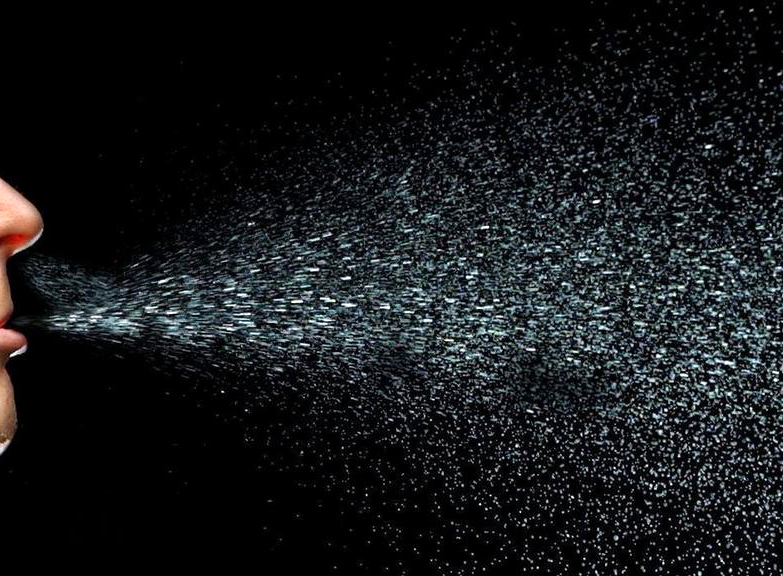
It causes coughing and thereby produces airborne droplets that contain bacterial cells and are likely to infect anyone inhaling them.
The incubation period for pneumonic plague is short, usually two to four days, but sometimes just a few hours.
The initial signs are indistinguishable from several other respiratory illnesses; they include headache, weakness, and spitting or vomiting of blood.
The course of the disease is rapid; unless diagnosed and treated soon enough, typically within a few hours, death may follow in one to six days; in untreated cases, mortality is nearly 100%.
♦ Cause
The bubonic and septicemic forms are generally spread by flea bites or handling an infected animal, whereas pneumonic plague is generally spread between people through the air via infectious droplets.
The Oriental rat flea (Xenopsylla cheopis) engorged with blood after a blood meal. This species of flea is the primary vector for the transmission of Yersinia pestis, the organism responsible for bubonic plague in most plague epidemics in Asia, Africa, and South America.
Both male and female fleas feed on blood and can transmit the infection.
A child bitten by a flea infected with the bacterium Yersinia pestis.
Y. pestis, a member of the family Yersiniaceae, has caused the bite to become ulcerated.
Transmission of Y. pestis to an uninfected individual is possible by any of the following means:
* droplet contact – coughing or sneezing on another person
* direct physical contact;– touching an infected person, including sexual contact
* indirect contact – usually by touching soil contamination or a contaminated surface
* airborne transmission – if the microorganism can remain in the air for long periods
* fecal-oral transmission – usually from contaminated food or water sources
* vector borne transmission – carried by insects or other animals.
Contrary to popular belief, rats did not directly start the spread of the bubonic plague.
It is mainly a disease in the fleas (Xenopsylla cheopis) that infested the rats, making the rats themselves the first victims of the plague.
Rodent-borne infection in a human occurs when a person is bitten by a flea that has been infected by biting a rodent that itself has been infected by the bite of a flea carrying the disease.
The bacteria multiply inside the flea, sticking together to form a plug that blocks its stomach and causes it to starve. The flea then bites a host and continues to feed, even though it cannot quell its hunger, and consequently, the flea vomits blood tainted with the bacteria back into the bite wound.
The bubonic plague bacterium then infects a new person and the flea eventually dies from starvation. Serious outbreaks of plague are usually started by other disease outbreaks in rodents or a rise in the rodent population.
♦ Diagnosis
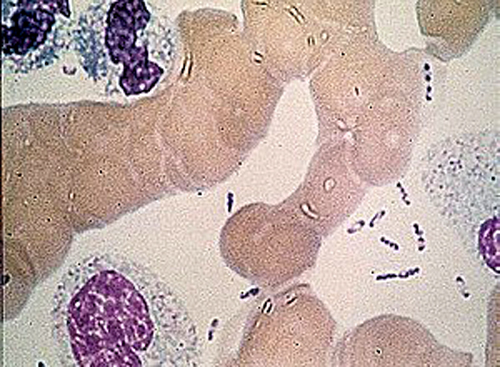
Diagnosis is typically by finding the bacterium in fluid from a lymph node, blood or sputum.
Y. pestis can be identified through both a microscope and by culturing a sample and this is used as a reference standard to confirm that a person has a case of plague.
The sample can be obtained from the blood, mucus (sputum), or aspirate extracted from inflamed lymph nodes (buboes).
If a person is administered antibiotics before a sample is taken or if there is a delay in transporting the person's sample to a laboratory and/or a poorly stored sample, there is a possibility for false negative results.
Polymerase chain reaction (PCR) may also be used to diagnose plague, by detecting the presence of bacterial genes such as the pla gene (plasmogen activator) and caf1 gene, (F1 capsule antigen).
PCR testing requires a very small sample and is effective for both alive and dead bacteria.
For this reason, if a person receives antibiotics before a sample is collected for laboratory testing, they may have a false negative culture and a positive PCR result.
Blood tests to detect antibodies against Y. pestis can also be used to diagnose plague, however, this requires taking blood samples at different periods to detect differences between the acute and convalescent phases of F1 antibody titres.
♦ Prevention
Vaccination
Since human plague is rare in most parts of the world as of 2023, routine vaccination is not needed other than for those at particularly high risk of exposure.
It is not even indicated for most travellers to countries with known recent reported cases, particularly if their travel is limited to urban areas with modern hotels.
The United States CDC thus only recommends vaccination for
(1) all laboratory and field personnel who are working with Y. pestis organisms resistant to antimicrobials
(2) people engaged in aerosol experiments with Y. pestis
(3) people engaged in field operations in areas with enzootic plague where preventing exposure is not possible (such as some disaster areas).
Early diagnosis
Diagnosing plague early leads to a decrease in transmission or spread of the disease.
Prophylaxis
Pre-exposure prophylaxis for first responders and health care providers who will care for patients with pneumonic plague is not considered necessary as long as standard and droplet precautions can be maintained.
In cases of surgical mask shortages, patient overcrowding, poor ventilation in hospital wards, or other crises, pre-exposure prophylaxis might be warranted if sufficient supplies of antimicrobials are available.
Postexposure prophylaxis should be considered for people who had close (<6 feet), sustained contact with a patient with pneumonic plague and were not wearing adequate personal protective equipment. Antimicrobial postexposure prophylaxis also can be considered for laboratory workers accidentally exposed to infectious materials and people who had close (<6 feet) or direct contact with infected animals, such as veterinary staff, pet owners, and hunters.
♦ Treatments
If diagnosed in time, the various forms of plague are usually highly responsive to antibiotic therapy.
The antibiotics often used are streptomycin, chloramphenicol and tetracycline.
Amongst the newer generation of antibiotics, gentamicin and doxycycline have proven effective in monotherapeutic treatment of plague.
Guidelines on treatment and prophylaxis of plague were published by the Centers for Disease Control and Prevention in 2021.
The risk of death with treatment is about 10% while without it is about 70%.
The plague bacterium could develop drug resistance and again become a major health threat. One case of a drug-resistant form of the bacterium was found in Madagascar in 1995.
Further outbreaks in Madagascar were reported in November 2014 and October 2017.
♦ Epidemiology
Globally about 600 cases are reported a year.
In 2017, the countries with the most cases include the Democratic Republic of the Congo, Madagascar and Peru.
♦ History
It has historically occurred in large outbreaks, with the best known being The Black Death in the 14th century which resulted in more than 50 million dead.
In 2022 the possible origin of all modern strands of Yersinia pestis DNA was found in human remains in three graves located in Kyrgyzstan, dated to 1338 and 1339.
The siege of Caffa in Crimea in 1346, is known to have been the first plague outbreak with following strands, later to spread over Europe.
♦ Biological weapon
The plague has a long history as a biological weapon.
Historical accounts from ancient China and medieval Europe details the use of infected animal carcasses, such as cows or horses, and human carcasses, by the Xiongnu/Huns, Mongols, Turks and other groups, to contaminate enemy water supplies. Han Dynasty General Huo Qubing is recorded to have died of such contamination while engaging in warfare against the Xiongnu.
Plague victims were also reported to have been tossed by catapult into cities under siege.
In 1347, the Genoese possession of Caffa, a great trade emporium on the Crimean peninsula, came under siege by an army of Mongol warriors of the Golden Horde under the command of Jani Beg.
After a protracted siege during which the Mongol army was reportedly withering from the disease, they decided to use the infected corpses as a biological weapon. The corpses were catapulted over the city walls, infecting the inhabitants.
This event might have led to the transfer of the Black Death via their ships into the south of Europe, possibly explaining its rapid spread.
During World War II, the Japanese Army developed weaponized plague, based on the breeding and release of large numbers of fleas.
During the Japanese occupation of Manchuria, Unit 731 deliberately infected Chinese, Korean and Manchurian civilians and prisoners of war with the plague bacterium.
These subjects, termed "maruta" or "logs", were then studied by dissection, others by vivisection while still conscious.
Members of the unit such as Shiro Ishii were exonerated from the Tokyo tribunal by Douglas MacArthur but 12 of them were prosecuted in the Khabarovsk War Crime Trials in 1949 during which some admitted having spread bubonic plague within a 36-kilometre (22 mi) radius around the city of Changde.
After World War II, both the United States and the Soviet Union developed means of weaponising pneumonic plague. Experiments included various delivery methods, vacuum drying, sizing the bacterium, developing strains resistant to antibiotics, combining the bacterium with other diseases (such as diphtheria), and genetic engineering.
The plague can be easily treated with antibiotics. Some countries, such as the United States, have large supplies on hand if such an attack should occur, making the threat less severe.
Plague
Related
References
https://en.wikipedia.org/wiki/Plague_(disease)
photo
large photo: Hans den Boer_ErasmusMC_Rotterdam

- Actinomycosis
- Anthrax
- Biopsy Sinusitis_Aspergillus flavus
- Botulism
- Brucellosis
- Cat Scratch Disease
- Cellulitis
- Cholera
- Creutzfeldt-Jakob Disease
- Cystic Fibrosis_CF
- Diphtheria
- Erysipelas
- Erysipeloid or fish poison
- Legionnaires disease
- Lemierre syndrome
- Leprosy
- Listeriosis
- Lyme / Borreliosis
- Melioidosis
- Meningitis
- Plague
- Syphilis
- Tetanus
- Trench Mouth_Plaut-Vincent_acute necrotizing ulcerative gingivitis
- Tuberculosis (TB)
- Tularemia_Rabbit Fever
- Typhoid fever (Epidemic typhus)
- Whooping Cough