




Methylobacterium rhodinum
-
General information
Taxonomy
Family: Methylobacteriaceae
Natural habitat
They are isolated mostly from vegetation, but may also occasionally be found in the hospital enviroment.
Tap water has been implicated as a possible agent of transmission in hospital environment.
Methylobacterium species are a cause of health care-associated infections, including infections in immunocompromised hosts.
The ability of Methylobacterium to form biofilms and to develop resistance to high temperatures, drying, and desinfecting agents may explain the colonization of Methylobacterium in the hospital environment in e.g. endoscopes.
Due to its slow growth, it can be easily missed during microbiological surveillance of endoscope reprocessing.
They are able to utilize methanol as a sole source of carbon and energy, although this characteristic may be lost on subculture.
Clinical significance
They have been reported to cause septicemia, continous ambulatory peritoneal dialysis related peritonitis, skin ulcers, synovitis, and other infections often in immunocompromised patients, as well as pseudoinfections.
-
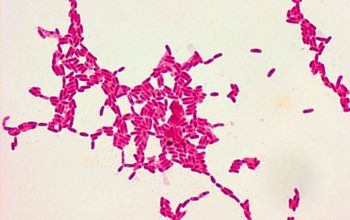
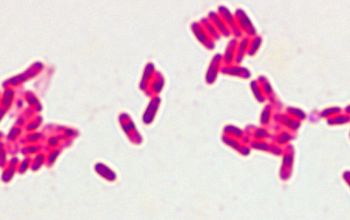
Gram stain
Gram-negative bacilli
Cells are pleomorphic, vacuolated rods that stain poorly and may resist decoloration
They have cell inlusions (sudanophilic)
-
Culture characteristics
-
Obligate aerobic
Optimum growth occurs between 25 and 30°C.
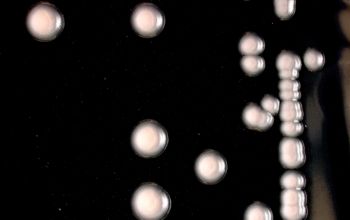
BA: growth is fastidious on ordinary media (like blood agar), producing 1 mm diameter colonies after 4-5 days.
They are very small, dry and coral pink.
Sabouraud / LEG-, R2A agar
Red colonies
MacConkey: no growth
UV-light
Colonies appear dark due to absorption of UV-light.
-
-
Characteristics
-
References
James Versalovic et al.(2011) Manual of Clinical Microbiology 10th Edition
Karen C. Carrol et al (2019) Manual of Clinical Microbiology, 12th Edition
Methylobacterium and Its Role in Health Care-Associated Infections Journal of Clinical Microbiology
Microbiology on the go. An initiative by
Dept. Medical Microbiology and Infectious diseases